


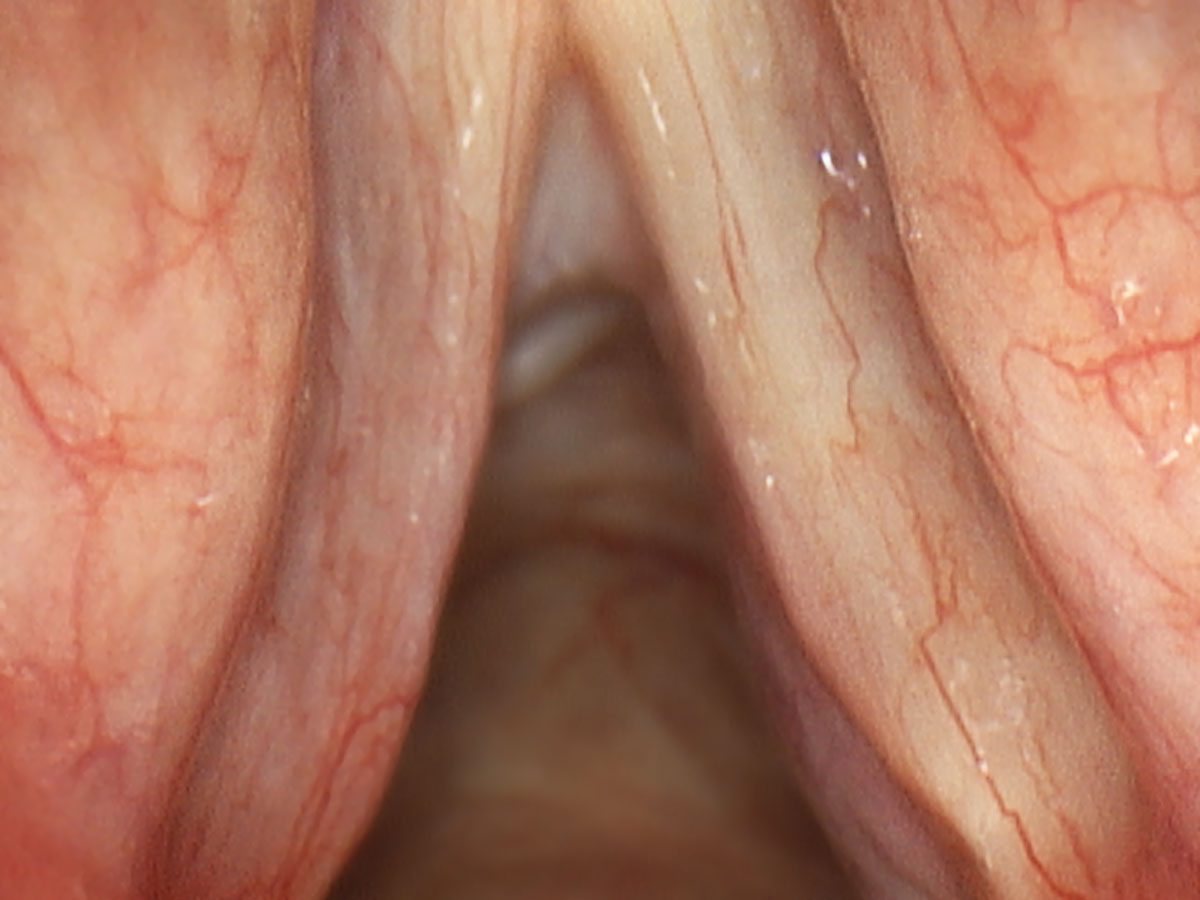

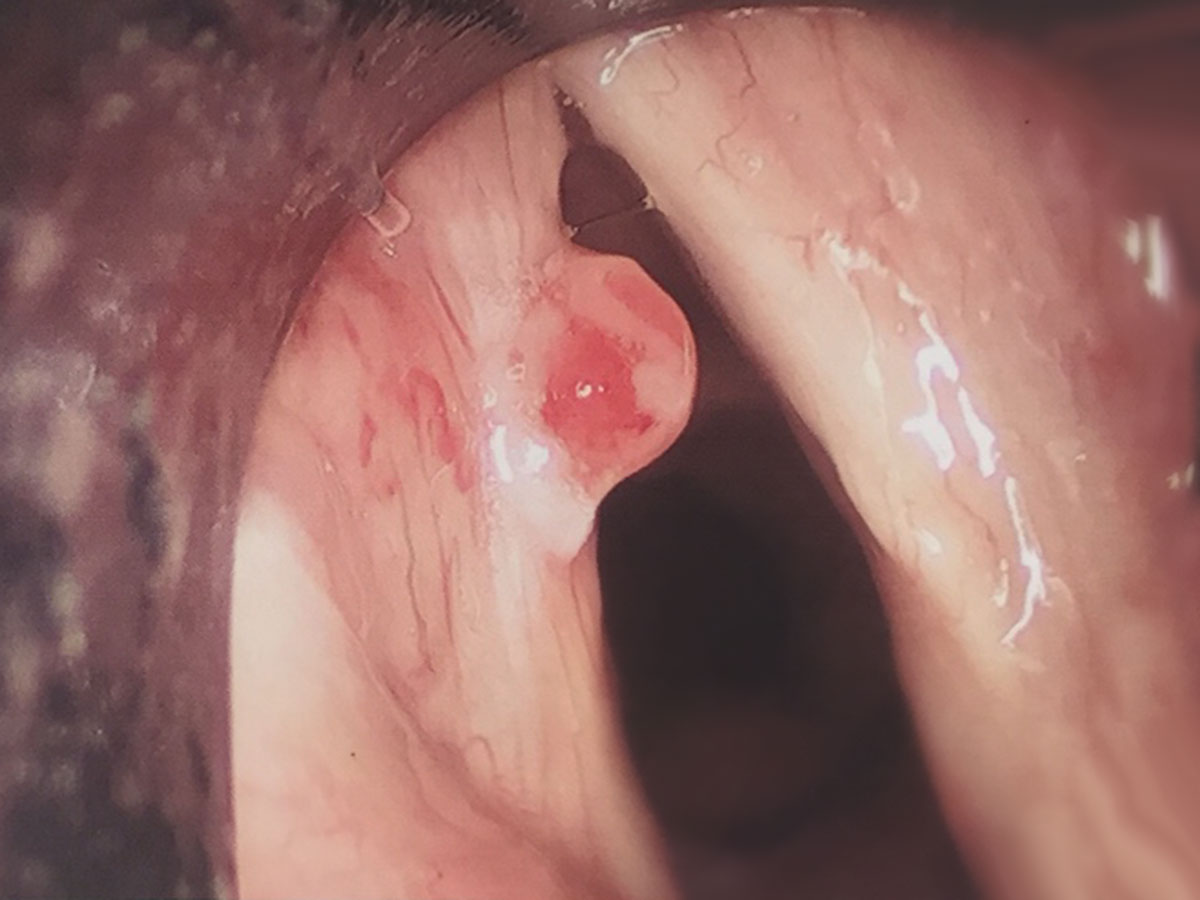

Larynx cancer fortunately is not particularly common in Australia. Over 80% of larynx cancers arise from the vocal fold. As such, most vocal cord cancers therefore present with hoarseness. It is current teaching at subspecialised laryngeal surgery centres that hoarseness persisting for more than three weeks should involve a laryngology review to ensure treatable diseases are not missed. Larynx cancer in its early stages (T1, T2, AJCC) traditionally was treated with external beam radiotherapy. This was a highly effective technique at curing early cancers of the vocal fold. It is still the most commonly used modality within Australia and in many parts of the world. The technology has certainly improved but it still uses ionising radiation to treat cancer and cannot be targeted solely to the cancer. As such, it also treats the viable healthy, non-cancerous tissue surrounding the tumour and as such, can cause significant morbidity. Typically, external beam radiotherapy destroys the mucous glands around the vocal cords causing permanent dryness and hoarseness to the speaking voice. It also damages the delicate layered microstructure of each vocal fold, again contributing to permanent hoarseness. Longer term effects of radiotherapy include difficulty swallowing, which is irreversible.
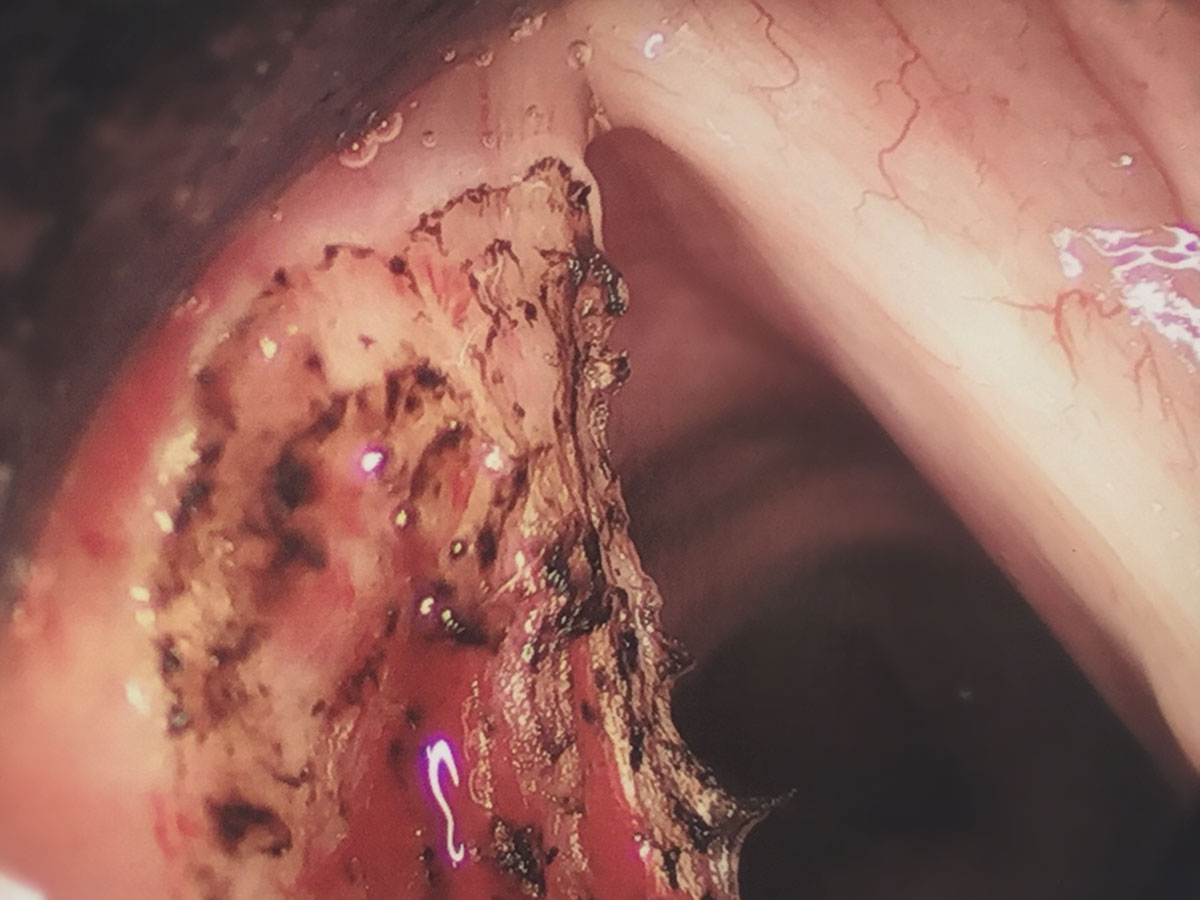
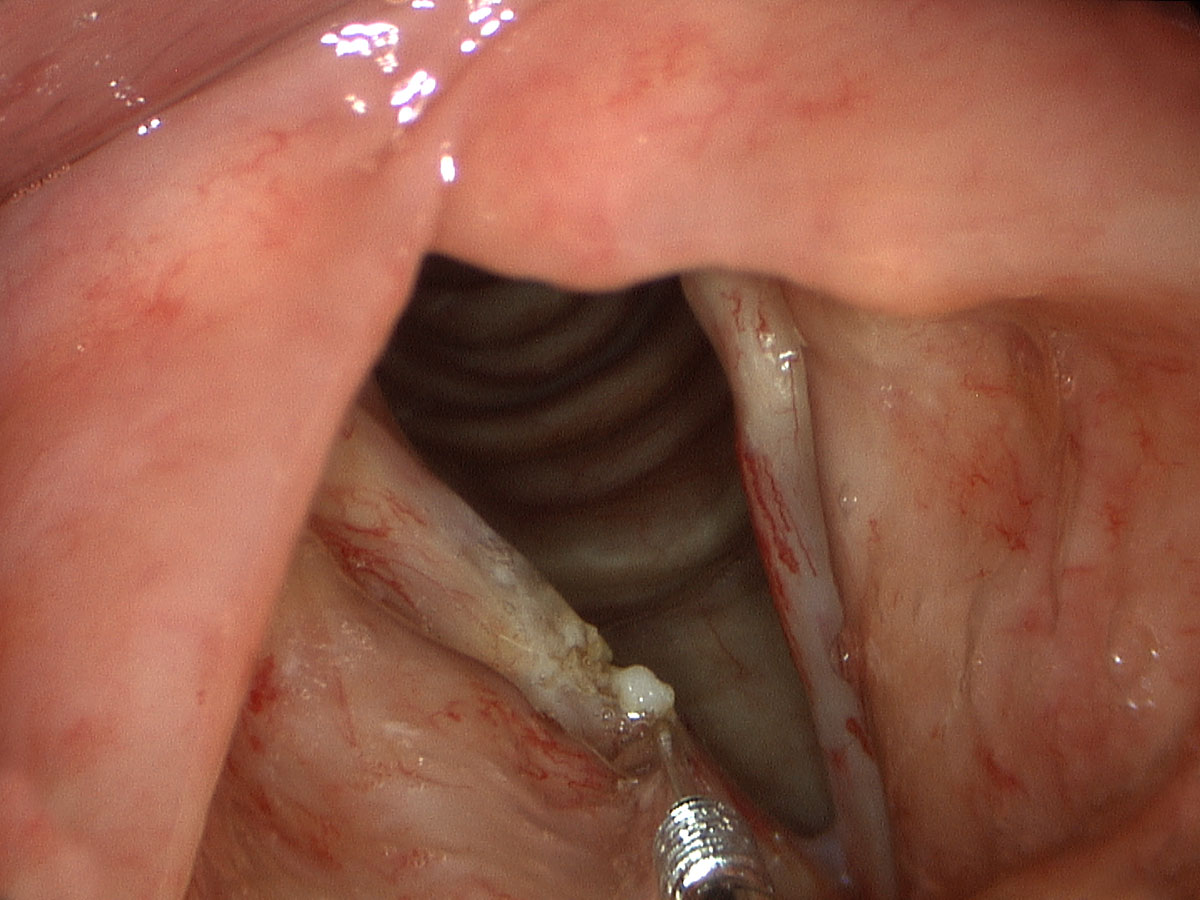
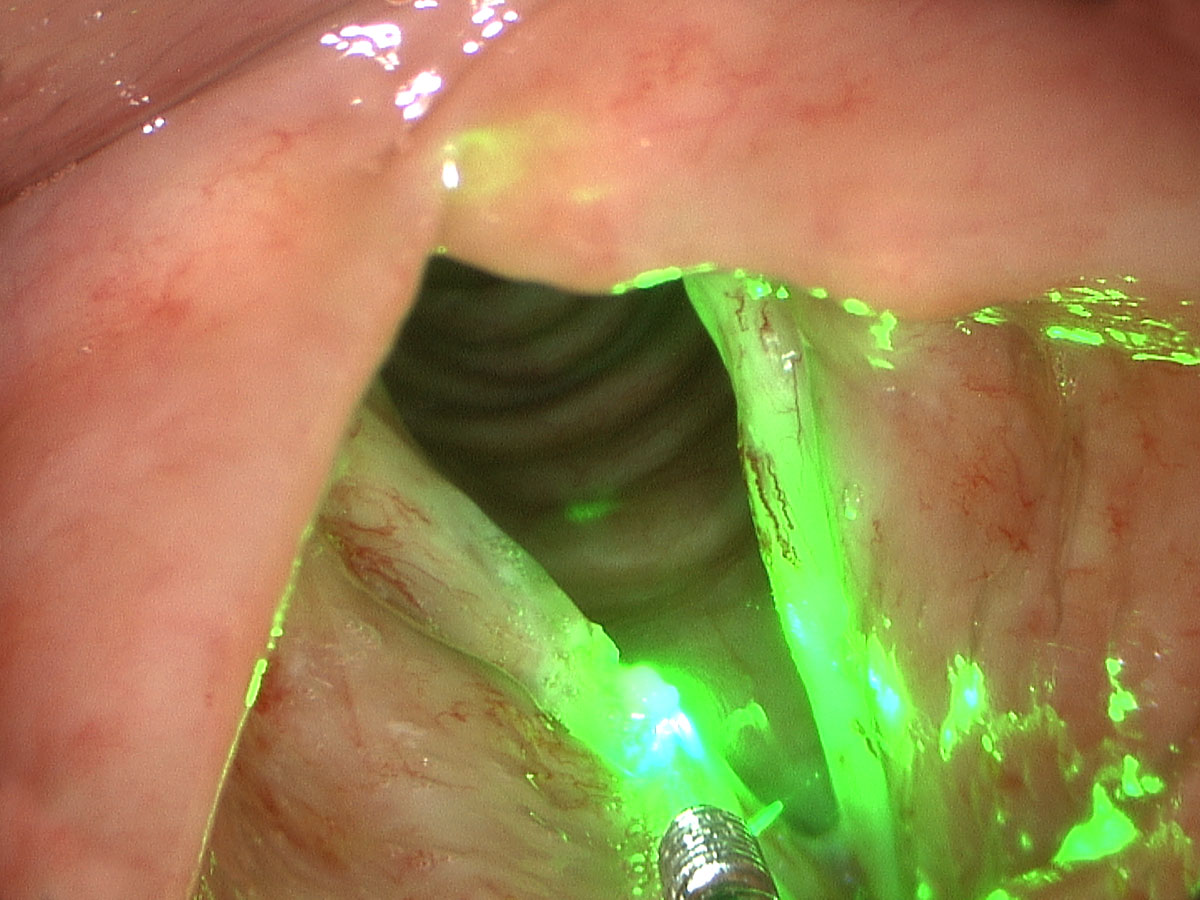
The other common modality for treating early glottic cancer is transoral laser microsurgery. In the majority of cases this utilises the carbon dioxide laser. The carbon dioxide laser is an effective laser at cutting tissue out but is not able to provide selective blood vessel ablation at the periphery of a tumour or treat surrounding pre-cancerous lesions without destroying healthy vocal cord tissue below. As such, some of the most innovative larynx cancer treatment centres utilise the newer, highly specific angiolytic lasers, including the KTP laser. At the Centre for Laryngeal Surgery and Voice Restoration in Boston, Massachusetts under Dr Zeitels, Dr Broadhurst learnt the techniques involved in angiolytic laser treatment for larynx cancer. In Boston over the last 10 years there have been hundreds of patients treated successfully with this technique establishing the KTP laser as a safe and effective treatment option for early glottic cancer. Results from the Boston group and Dr Broadhurst’s own results, having since being established back in Australia, have shown comparable cure rates and disease control rates to both radiotherapy and CO2 laser excision. In contrast however, they have shown substantially better voice outcomes for patients. If one considers that all treatment modalities are equivocal in their ability to control or cure disease, then the most important metric of success becomes the voice outcome. Given the unique interaction of the KTP laser with both the cancer and the surrounding pre-cancerous tissue, the angiolytic KTP laser provides a substantial advantage in voice preservation in managing these lesions.
Recently in July 2015 at the World Larynx Cancer Congress, Dr Broadhurst was an invited speaker for numerous talks on the efficacy of the KTP laser in treating early glottic cancer.
